


TMJ/ Myofacial
Pain
COMPUTERIZED
DIAGNOSTICS: The Key to Success
WHAT IS
"TMJ'? - Parker E. Mahan, DDS, PhD, Professor and Chairman
According to the National Institutes of Health, Temporomandibular Disorders
refer to a collection of medical and dental conditions affecting the
temporomandibular joint and/or the muscles of mastication (chewing muscles), as
well as related tissue components.
"The TMJs are the two joints in the front of the ears that attach the lower
jaw (mandible) to the skull (fossa). Not only do the jaw joints rotate as other
ball-and-socket joints, they translate (move down and forward). The disc (articular
disc) is a thin piece of tissue acting as a buffer between the skull and the
condyle (top of the mandible).
When intact, they are the only joints in the human body that work together as a
unit. These joints, often taken for granted, allow us to perform functions as
opening and closing the mouth, chewing, swallowing, breathing, kissing, talking,
etc. Problems that can occur with the temporomandibular joint are arthritis,
trauma, tumors, tearing or dislocation of the disc. The TMJs and the mandibular
complex are able to function and move by means of innervated muscle, tissue, and
ligaments that are the connecting components between the lower jaw (the
mandible) and the skull (cranium). There often can be accompanying muscle spasms
that effect temporomandibular diseases/disorders which often are diagnosed as
Fibromyalgia or Myofacial Pain Dysfunction. You may experience joint problems,
muscle problems or both.
Numerous Signs and
Symptoms
"TMJ" as we know it presents with numerous signs and symptoms which
include: a clicking or popping jaw and mild discomfort to complete jaw
dysfunction and severe debilitating pain. Many can experience a varying
combination of these symptoms with varying degrees of discomfort. Many discover
that these symptoms may be transient and go away on there own with or without
treatment. However, for many others, it can be the beginning of a long,
agonizing and frustrating life where lives are disrupted, dreams shattered,
families torn apart and people left bankrupt, desperate and without hope. If you
have TMJ, you may have spent years of your life and thousands of dollars being
referred from one doctor to another hoping for relief. Doctors may have told you
that you are crazy or need to better handle your stress. They may have told you
that you don't have pain. They may even have abandoned you, saying there is
nothing more to be done for you...that is, after you have spent thousands or
hundreds of thousands of dollars on treatments.
If this sounds familiar, you are not alone. You are not crazy and you are not to
blame if you haven't gotten better. It is possible that you have received one or
many of the over 49 treatments being recommended to TMJ patients in this
country, most being sold on the basis of the doctor's preference, not
scientific evidence of safety or effectiveness. The treatment may, in fact,
be making you worse. You may feel caught in a quagmire. Your personal experience
may be that there is a great deal of disagreement among professionals about most
aspects of temporomandibular joint diseases/disorders.
SYMPTOMS
The symptoms most commonly cited are as follows:
This list of subjective symptoms is by no means exhaustive, but does provide a
good idea of the nature of the complaints that are often made by those suffering
from TMD.
Diagnostic Classification
The NIH Technology Assessment Conference Statement concludes, "there are
significant problems with present diagnostic classifications of TMD, because
these classifications appear to be based on signs and symptoms rather than on
etiology." They further state that, "...scientifically based
guidelines for diagnosis ... are still unavailable."
"One of the most difficult and controversial diagnoses the practicing
dentist must make is that of the temporomandibular joint dysfunction syndrome (MPD).
Controversy still abounds in our literature and at professional meetings even
though almost all involved therapists agree that head and neck muscles are
affected in the syndromes. The champions of each concept of etiology tend to
ignore or belittle the conflicting concepts as though there can be only one
cause of TMJ-MPD problems."
The dental community usually diagnoses TMJ based on several things, including
range of motion tests, listening for sounds in the joints, examining the teeth,
and palpation of the jaw joints as well as the muscles of the face, and head.
Typically the dentist will ask for information about your pain and other
symptoms, injuries, oral habits, and previous medical and dental treatment.
Department of Basic Dental Sciences, University of Florida, Gainesville,
Florida
HOW MANY PEOPLE HAVE
"TMJ"? WHO GETS IT?
According to the National Institutes of Health, over ten million Americans
suffer from TMJ Diseases/Disorders. This is the most conservative estimate we
have seen.
Both males and females can get TMJ diseases/disorders. However, 90% of those
seeking treatment for TMJ are women, most between puberty and menopause. Recent
research has focused attention on the relationship between sex hormones and
pain. A study conducted by Dr. Linda LeResche, University of Washington in
Seattle, demonstrated that women on hormone replacement therapy were 77% more
likely to seek treatment for jaw pain than those not undergoing such treatment.
Also, women on oral contraceptive therapy were 19% more likely to seek
treatment. Evidence is emerging in support of a biological explanation for why
there are more women suffering from TMJ pain.
A study done by Dr. Peter Waite, University of Alabama at Birmingham
"demonstrates a high incidence of TMJ dysfunction among Mitral Valve
Prolapse patients and leads to a suspicion of a common connective tissue
disorder." In an unrelated survey conducted by the Society for Mitral Valve
Prolapse Syndrome, of 240 patients surveyed 51% had also been diagnosed with
TMJ.
A recent study conducted by Dr. J.C. Turp found that among a great percentage of
TMJ patients the pain distribution was more widespread than commonly assumed.
"Evidence suggests a significant overlap between temporomandibular disorder
states and pain conditions in other parts of the body".
Consult Your Medical
Doctor
We recommend that you first consult with a medical doctor to rule out any
disease that may be causing your symptoms and is treated by medical
practitioners. If they are unable to find a reason for your problem, and you are
referred to a dentist for a TMJ evaluation, we encourage you to then obtain
multiple INDEPENDENT opinions on your condition.
Get an Independent Opinion
To be a truly independent opinion, the medical/dental professional can not be
associated with or working with the medical/dental professional from whom you
have already received an opinion. Many TMJ patients seek further opinions
outside of their geographical area, without the referral of their original
medical/dental professional.
Educate Yourself and
Others
With the increase of managed care (HMOs), where a primary care physician is your
health care gatekeeper it is mandatory that you, the patient, become your own
well-informed advocate. You will also need to educate your primary care
physician and all others you encounter within the system about TMJ.
As the Washington Post states in their Health News section on May 7, 1996, this
is critical for " ...medical science is so uncertain about how to treat jaw
pain because the disorder has not been accurately diagnosed or described - and
no one is sure whether it should be treated by doctors or dentists, or
both." For additional information on treatment modalities and problems see
our section on Treatments.
Musculoskeletal
Dysfunction (MSD) of the Head and Neck Resulting in
Temporomandibular (Jaw) Joint Dysfunction ("TMJ")
(Some portions of the following section contains excerpts of writings from Dr. James Garry, who is an expert in treating musculoskeletal dysfunctions of the head, neck and temporomandibular joint dysfunction as well as air-way obstruction/ sleep apnea problems).
Patients suffering facial pain, headaches, neck
aches, shoulder, and/ or back pain often have to learn to live with the pain.
Some patients have subjective hearing loss, ringing of the ears, dizziness, pain
in the ear, a feeling of fullness or pressure in the ears, clicking/ popping of
the jaw joints and eye pain. The mouth, teeth and throat may also be affected. When
competent clinicians cannot find an organic basis for these symptoms, they often
suggest it might be psychogenic.
There is a classification of disease known as Musculoskeletal Dysfunction of
the head and neck (MSD). MSD seems totally unrelated to symptoms such as
back pain or ear disorders. Yet, correction of this condition may alleviate many
medical symptoms; acute or chronic diseases of the ear, nose, throat, head,
neck, shoulder and back. The syndrome is medically as well as dentally
related.
TMJ/ MSD is a dysfunction of a group of associated muscles, ligaments, nerves
and supportive structures that are associated with the temporomandibular joint.
Unfortunately, TMJ/ TMD is one of the most misdiagnosed of the medical/ dental
conditions. There are two aspects that contributes to this sad phenomenon of
misdiagnosis.
First, few doctors including physicians, ENT specialists, dentists,
chiropractors, osteopaths, etc. have a comprehensive understanding and
perspective in the diagnosis and treatment of TMJ/ MSD.
Secondly, these disorders have many overlapping symptoms which mimic many other
conditions such as neurological disorders, ringing and fullness in the ear,
headaches, etc.
Misdiagnosis is the rule rather than the exception with MSD. Patients
wander from specialist to specialist, depending on the type of pain and problems
they experience. Symptoms focusing on ear, sinuses, or swallowing problems are
referred to the Otolaryngologist. Limitations of jaw movement are referred to
the Orthopedist. Persistent head pains are referred to the Neurologist, etc.
As the wanderers are told and retold that there seems to be no organic basis for
their pain, that the cause is psychogenic, their anxiety mounts. When physical
findings remain obstinately in abeyance, patients may begin to suspect a brain
tumor, turn to drugs to alleviate their symptoms, or on rare occasions, even
contemplate suicide.
ANATOMY OF TEMPOROMANDIBULAR JOINT:
The Temporomandibular Joint is the joint connecting the jaw (mandible) to the
skull (temporal bone).
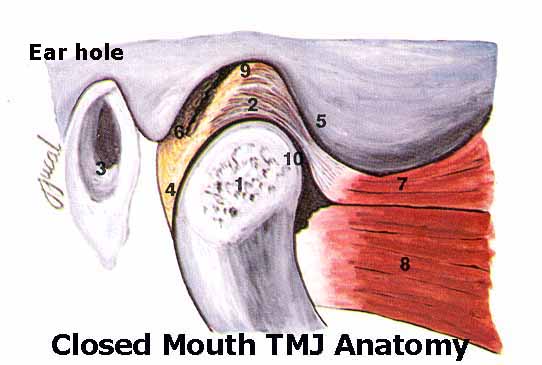 The two bones are held together and function via a complex group of muscles,
ligaments and other soft tissue. The temporal bone has a concavity call the
glenoid fossa in which the head of the jawbone (the condyle)sits. A cartilage
disc call the articular disc separates the two bones. The articular disc slides
in conjunction with the mandible to provide smooth quiet movement and acts as a
cushion against heavy forces generated by the strong jaw muscles. The right and
left TMJ joints do not act as a separate joints, but must move in coordination
with one another.
The two bones are held together and function via a complex group of muscles,
ligaments and other soft tissue. The temporal bone has a concavity call the
glenoid fossa in which the head of the jawbone (the condyle)sits. A cartilage
disc call the articular disc separates the two bones. The articular disc slides
in conjunction with the mandible to provide smooth quiet movement and acts as a
cushion against heavy forces generated by the strong jaw muscles. The right and
left TMJ joints do not act as a separate joints, but must move in coordination
with one another.
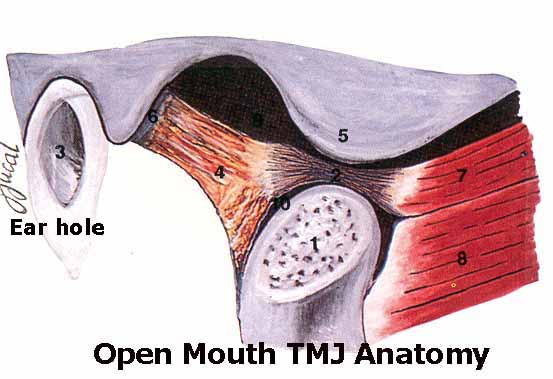 The TMJ joints are considered the most complex joints in the human body because
they must provide for rotational movements, sliding movements and an infinite
range of combined movements and functions, unlike any other joint in the body.
The TMJ joints are considered the most complex joints in the human body because
they must provide for rotational movements, sliding movements and an infinite
range of combined movements and functions, unlike any other joint in the body.
The lower jaw (Mandible) has a relationship to the upper jaw (Maxilla). If
this relationship is altered, the muscles of mastication (chewing muscles) go
into spasm. This causes the muscles that have the same nerve intervention to
also go into spasm. The resulting stresses may radiate throughout the head,
neck, and even involve the back. The pain may be constant or intermittent,
lasting minutes, hours, days, or even years. Many patients describe the pain as
a migraine headache. Eventually a patient may demonstrate clicking, grating,
snapping, or popping sounds in the joint.
MECHANICS OF TEMPOROMANDIBULAR JOINT DYSFUNCTION:
The lower jaw may be over closed (too close to the upper jaw), and /or distally
displaced (too far back in the joint or socket). Also, the lower jaw may deviate
to one side due to interfering tooth cusps (points on the chewing surfaces of
teeth that do not meet properly with the opposing teeth).
The cause is multifaceted, i.e., loss of teeth, poor alignment or natural
wear of teeth, grinding or clenching of the teeth day and night, poor tongue
position, a muscle imbalance in the tongue and the facial muscles, chronic mouth
breathing, osteoarthritis, rheumatoid arthritis, trauma, etc.
To determine if an improper relationship exists between upper arch and the lower
jaw, it is necessary to relax the muscles of mastication (chewing muscles), then
close the relaxed lower jaw on a trajectory that is not strained. In other
words, the mouth closes where the muscles are most comfortable.
To relax the muscles of mastication, a gentle pulsating stimulus is applied to
the skin for approximately one hours. Multi-channel electromyography (EMG) is
used to verify the degree of muscular relaxation.
MSD is not a rare condition. Every patient has some degree of Musculoskeletal
dysfunction. It is when symptoms are manifested that people seek help. Many
patients tend to clench and/or grind their teeth in response to unconscious
stress, creating muscular dysfunction. This usually occurs during sleep, but it
may also occur during a stressful daily experience. Resolution of unconscious
stress which cause symptoms indicated on the Screening questionnaire may require
stress counseling. Subconscious stress must be controlled for successful
resolution of clenching and /or grinding of teeth.
POSTURE AND AIRWAY
Posture has an effect on the relationship of the lower jaw to the cranium and
can result in a malocclusion (improper bite). If body symmetry is not within
normal limits, physical therapy may be necessary to correct body symmetry during
treatment.



Airway obstruction must be cleared as it will result in constant mouth breathing. Allergy is a primary cause of chronic mouth breathing. If nasal obstruction is evident, consultation with an allergist and/or Otolaryngologist will be recommended during treatment. All chronic mouth breathers develop an improper bite (malocclusion).
INITIAL TREATMENT FOR TMJ:
Three approaches or a combination thereof, may be recommended as initial therapy:
1. Occlusal correction or coronoplasty (reshaping teeth to remove interferences that cause abnormal jaw displacement).
2. Construct an orthotic to orthopedically align the lower jaw to the cranium in three dimensions providing there is an over closure. If symptoms subside after wearing the appliance for three months, crowns may be recommended to maintain the orthopedic position established by the orthotic. Orthododontia may be recommended to avoid crowns. Possibly a combination of orthodontia and crowns will be recommended. When posterior (back) teeth are missing, dentures and /or partials may be recommended. For more details, see OUR TREATMENT PROTOCOL
3. Surgery is the last and least recommended when irreversible damage has occurred in the joints and is beyond natures healing capacity.